

The recent news about the opening of Carepoint Consumption and Treatment Service in London, Ontario signaled a new beginning after a long journey for the clients of the Temporary Overdose Prevention Site (TOPS), their care providers and advocates of supervised consumption and harm reduction sites more generally.
In an effort to understand the human impacts of the site on those who used the facility, a collaborative project was undertaken by researchers from CRHESI and the Middlesex London Health Unit (MLHU). Team members were former CRHESI Academic Director, Helene Berman, Michelle Sangster Bouck (MLHU), Abe Oudshoorn (Western), Melissa McCann (MLHU), Shamiram Zendo (Western), Jordan Banninga (MLHU), Marlene Janzen Le Ber (Brescia) and Zayya Zendo (Western).
This project could not have been carried out without the active involvement and generosity of the clients and service providers of Carepoint (formerly TOPS). Research findings showed that permanent, dignified and equitable health and social care services for people who use drugs is not only possible but saves lives.
Read my e-chat with researcher Abe Oudshoorn below.
Christine: Why did this issue become important to you when it did? What kinds of problems had you been seeing?
Abe: The devastating impact of drug poisonings in the London community (and communities across Canada) dates to well before the pandemic. Personally, I have been a life-long advocate of harm reduction approaches, and within the team at CRHESI we are passionate about equity approaches. When it comes to overdose prevention sites, we already have a lot of good data and evidence regarding the positive health benefits (and related cost benefits) from both research and organizational data. At this point, I didn’t see a huge need to once again show numbers that prove that overdose prevention sites save lives, reduce disease, and support people into other forms of treatment. Rather, for me what had been missing is the human story of how these sites exist within the daily lives of those who are most marginalized. The debate was almost detached from the human reality and we wanted to do work that put those who use the site front and centre. The hope was that having a platform for people to tell their stories would be impactful at the level of stigma and perceptions, thereby creating a more positive environment for good policy support.
Christine: What kind of influence has this research had on the research participants (people who use drugs) and on the community?
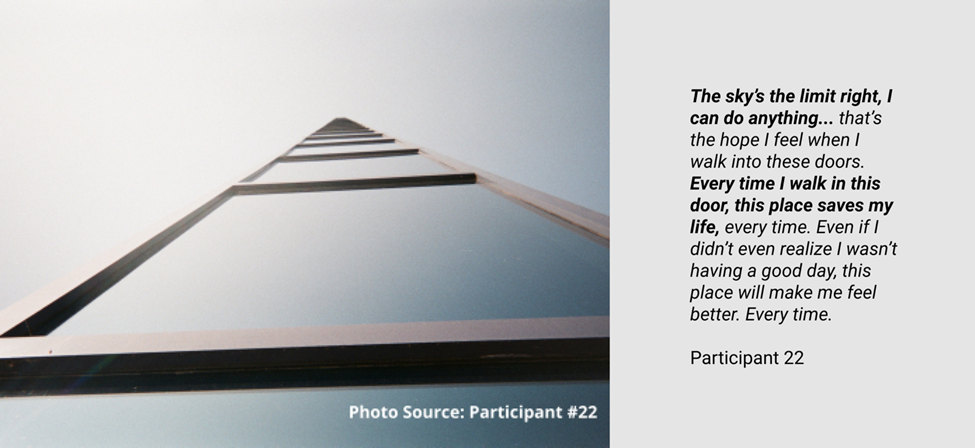
Abe: Using a photo method engaged the participants in a very rich way with the work. I have to give full credit to our team of Research Assistants and MLHU staff co-researchers who spent countless hours going to the site, meeting with people, supporting them in the photo taking, and exploring the meanings of the photos with them. The photos themselves tell a story, but the process of taking the photos and discussing them helps people elaborate on their experiences in ways they might otherwise find difficult. The richness of what participants were able to share is what I feel makes this work so impactful. I think we really need to lean into arts-based and relational approaches if we are going to be true to the idea of centring lived experiences in knowledge creation.
Christine: What do you think the London community may not understand about this issue? What did you learn that surprised you?
Abe: The most fundamentally meaningful finding from this work is that these sites are just disease-preventing, rather they have to potential to be transformational in the lives of people they support. The public narrative and perception around this work is still so often that harm reduction and recovery sit as some sort of poles, potentially opposed to each other. That it’s some sort of either/or. Instead, what we hear from the stories of our participants is that harm reduction delivered in a site where people are respected, welcomed, engaged, and supported is or can be part of a recovery journey. Not that everyone who uses an overdose prevention site regularly will then transition into some formalized treatment program, but by coming to this site they were just seeking survival but instead also found deep value and belonging. These human connections did translate for some participants into more formalized recovery in terms of managing substance use in safer ways or accessing specific programs/supports. But for all, with substance use rooted in deep disconnection, at the site they found connection that was transforming the very cause of their social distress. We don’t really think about overdose prevention sites like that, we tend to think of them as just some sort of quick, medical intervention. As is the fourth theme profiled in our work, they are actually transforming lives.
Christine: What’s next in addressing this issue? What are system level solutions?
Abe: Going forward, I think the tough thing we have to face as those who promote evidence-based solutions to complex challenges like substance use, is a shift in many provinces in Canada to politics over evidence. We are seeing some backlash and retraction of services especially in Central Canada, and those same pressures are being felt in Ontario, although so far the services continue largely unimpeded. To me, between the more clinical evidence and this work, the more human evidence, going forward the work needs to focus on knowledge mobilization and critical policy analysis. We need to translate this knowledge both with the public and with policy makers to ensure that governments are not perpetuating harms through partisan decision-making. This is tough work for academia where removal from controversy can be a lot safer, but if we can’t address urgent health issues in real-time then it feels to me like we’re missing the boat?
Hopefully we can be the bridge between those who are suffering and those who make the policy decisions to either alleviate or perpetuate their suffering.
With thanks to Abe for this interview
Abe Oudshoorn, RN, PhD is an Associate Professor in the School of Nursing at Western University and the Arthur Labatt Family Chair in Nursing Leadership in Health Equity. Having worked as a nurse with people experiencing homelessness, Dr. Oudshoorn’s research focuses on health equity through housing stability. Dr. Oudshoorn is past chair of the London Homeless Coalition and Managing Editor of the International Journal on Homelessness.
- Carepoint’s website lists service details.
- The Beyond Enduring study’s website has more detail about the study methods and outcomes.
- CRHESI’s Research Snapshot provides details about the study.
- MLHU has comprehensive evaluation reports about TOPS.
- Local news covered Carepoint’s opening at its permanent location.
- CRHESI’s blog explores substance use stigma and ways health and social service providers can improve care.